The thymus gland is a pink, lobulated lymphoid organ, located in the thoracic cavity and neck. In the adolescent, it is involved the development of the immune system. After puberty, it decreases in size and is slowly replaced by fat.
Embryologically, the thymus gland is derived from the third pharyngeal pouch.
In this article, we shall look at the anatomy of the thymus gland – its structure, position and vasculature.
Anatomical Structure and Position
The thymus gland has an asymmetrical flat shape, with a lobular structure. The lobules are comprised of a series of follicles, which have a medullary and cortical component:
- Cortical portion – Located peripherally within each follicle. It is largely composed of lymphocytes, supported epithelial reticular cells.
- Medullary portion – Located centrally within each follicle. It contains fewer lymphocytes than the cortex, and an increased number of epithelial cells. Hassall’s corpuscles are also present – these are concentric arrangements of epithelial reticular cells. Their function is unclear.
The gland is mainly located within the thoracic superior mediastinum, posterior to the manubrium of the sternum. However, in some individuals, it can extend superiorly into the neck (reaching the thyroid gland), and inferiorly into the anterior mediastinum (lying in front of the fibrous pericardium).
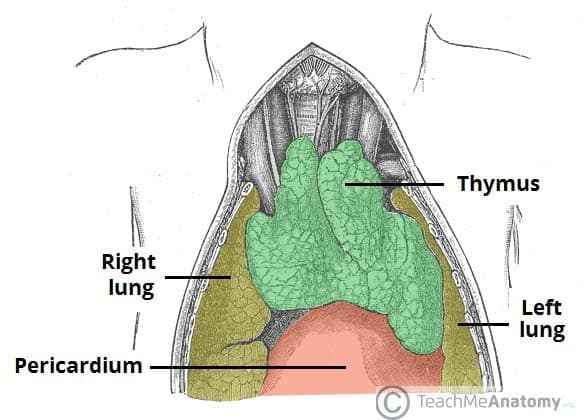
Fig 1.0 – The anatomical position of the thymus in the superior mediastinum.
Vasculature
The arterial supply to the thymus gland is via the anterior intercostal arteries and small branches from the internal thoracic arteries. Venous blood drains into the left brachiocephalic and internal thoracic veins.
Clinical Relevance: DiGeorge Syndrome
DiGeorge syndrome is a genetic syndrome caused by the deletion of part of chromosome 22. The clinical findings vary greatly between individuals. The most common features of the syndrome can be memorised using the mnemonic ‘CATCH’:
- Congenital heart defects
- Abnormal facies
- Thymic aplasia
- Cleft palate
- Hypoparathyroidism.
Individuals with an absent or asplastic thymus are susceptible to recurrent infections due to an underdeveloped immune system.