A myotome is defined as ‘a group of muscles innervated by a single spinal nerve root‘. They are clinically useful as they can determine if damage has occurred to the spinal cord, and at which level the damage has occurred.
In this article we shall look at the embryonic origins of myotomes, their distribution in the adult and their clinical uses.
Origin of Myotomes
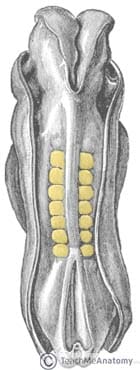
Skeletal muscle development can be traced to the appearance of somites. By day 20 the trilaminar disc has formed and the mesoderm has differentiated into different areas. The area directly adjacent to the neural tube is known as the paraxial mesoderm.
From day 20 onwards the paraxial mesoderm begins to differentiate further into segments known as somites. 44 pairs of somites are formed, however some of these regress until 31 pairs remain, corresponding to 31 pairs of spinal nerves in the adult.
Somites are composed of a dorsal and ventral portion. The ventral portion forms the sclerotome, the precursor of the ribs and vertebral column. The dorsal portion consists of the dermomyotomes. As the embryo continues to develop the myotome proliferates and eventually develops into muscle.
Distribution of Myotomes
Most muscles in the upper and lower limbs receive innervation from more than one spinal nerve root. They are therefore comprised of multiple myotomes.
For example, the biceps brachii muscle performs flexion at the elbow. It is innervated by the musculocutaneous nerve, which is derived from C5-7 nerve roots. All three of these spinal nerve roots can be said to be associated with elbow flexion.
The table below details which movement is most associated with each myotome:
| Upper Limb | Lower Limb |
|
|
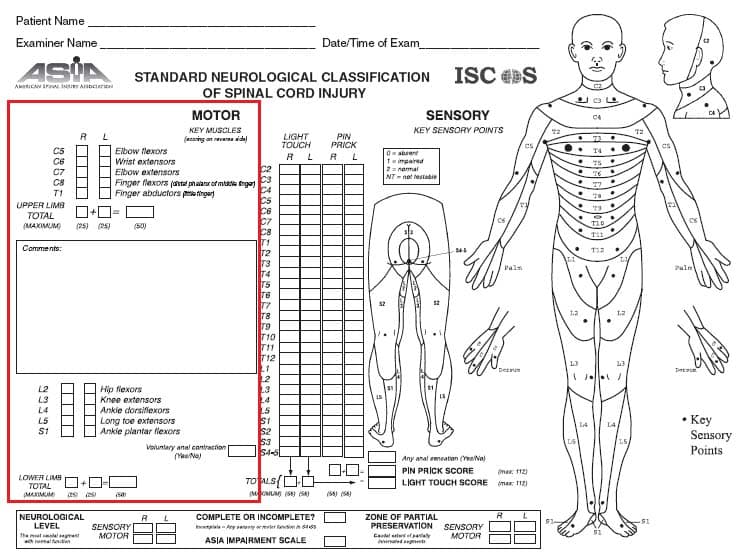
Clinical Relevance: Assessing Spinal Cord Lesions
In the assessment of a suspected spinal cord lesion, the clinician can test myotome function. This can help determine if there is spinal cord damage, and where the damage is located.
Myotomes are tested in terms of power, and graded 1-5:
- 0 = total paralysis.
- 1 = palpable or visible contraction.
- 2 = active movement, full range of motion (ROM) with gravity eliminated.
- 3 = active movement, full ROM against gravity.
- 4 = active movement, full ROM against gravity and moderate resistance in a muscle specific position.
- 5 = (normal) active movement, full ROM against gravity and full resistance in a muscle specific position expected from an otherwise unimpaired person.