The tibial nerve is a major peripheral nerve of the lower limb. It has several cutaneous and motor functions in the leg and foot.
In this article, we shall look at the anatomy of the tibial nerve – its anatomical course, functions and clinical correlations.
Overview
- Nerve roots: L4-S3
- Sensory: Innervates the skin of the posterolateral leg, lateral foot and the sole of the foot.
- Motor: Innervates the posterior compartment of the leg and the majority of the intrinsic foot muscles.
Anatomical Course
The tibial nerve is a branch of the sciatic nerve, and arises at the apex of the popliteal fossa. It travels through the popliteal fossa, giving off branches to muscles in the superficial posterior compartment of the leg. Here, the tibial nerve also gives rise to branches that contribute towards the sural nerve, which innervates the posterolateral aspect of the leg.
The tibial nerve continues its course down the leg, posterior to the tibia. During its descent, it supplies the deep muscles of the posterior leg.
At the foot, the nerve passes posteriorly and inferiorly to the medial malleolus, through a structure known as the tarsal tunnel. This tunnel is covered superiorly by the flexor retinaculum. Within this tunnel, branches arise from the tibial nerve to supply cutaneous innervation to the heel
Immediately distal to the tarsal tunnel, the tibial nerve terminates by dividing into sensory branches, which innervate the sole of the foot.
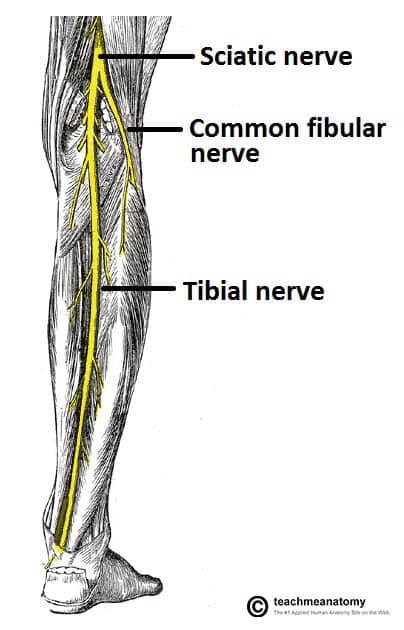
Fig 1 – Posterior view of the leg, with the superficial muscles removed. Anatomical course of the tibial nerve shown.
Clinical Relevance: Tarsal Tunnel Syndrome
Tarsal tunnel syndrome refers to entrapment and compression of the tibial nerve as it passes through the tarsal tunnel.
Patients may experience altered sensation in the sensory distribution of the tibial nerve – the sole of the foot.
The motor function of the nerve can also be affected in severe disease, causing weakness and wasting of the intrinsic foot muscles.
The management of tarsal tunnel syndrome can be conservative or surgical:
- Conservative: Physiotherapy, NSAIDs, corticosteroid injections
- Surgical: Tarsal tunnel release (cutting through the flexor retinaculum to decompress the tarsal tunnel)
Motor Functions
The tibial nerve innervates the muscles of the posterior leg and the majority of the intrinsic foot muscles.
Posterior Compartment of the Leg
The muscles of the posterior compartment of the leg are organised into a superficial and deep compartment. They are all innervated by the tibial nerve.
- Superficial:
- Plantaris – plantarflexion of the ankle.
- Soleus – plantarflexion of the ankle.
- Gastrocnemius – flexion of the knee and plantarflexion of the ankle.
- Deep:
- Popliteus – “unlocks” the knee by laterally rotating the femur on the tibia.
- Flexor hallucis longus – flexion of the great toe and plantarflexion of of the ankle
- Flexor digitorum Longus – flexion of digits 2-5 and plantarflexion of the ankle.
- Tibialis posterior – inversion of the foot and plantarflexion of the ankle.
Intrinsic Foot
The medial and lateral plantar branches of the tibial nerve provide innervation to the intrinsic muscles of the foot (exept the extensor digitorum brevis and extensor digitorum hallucis – which are innervated by the deep fibular nerve).

Fig 2 – Muscles in the deep layer of the posterior leg are innervated by the tibial nerve
Sensory Functions
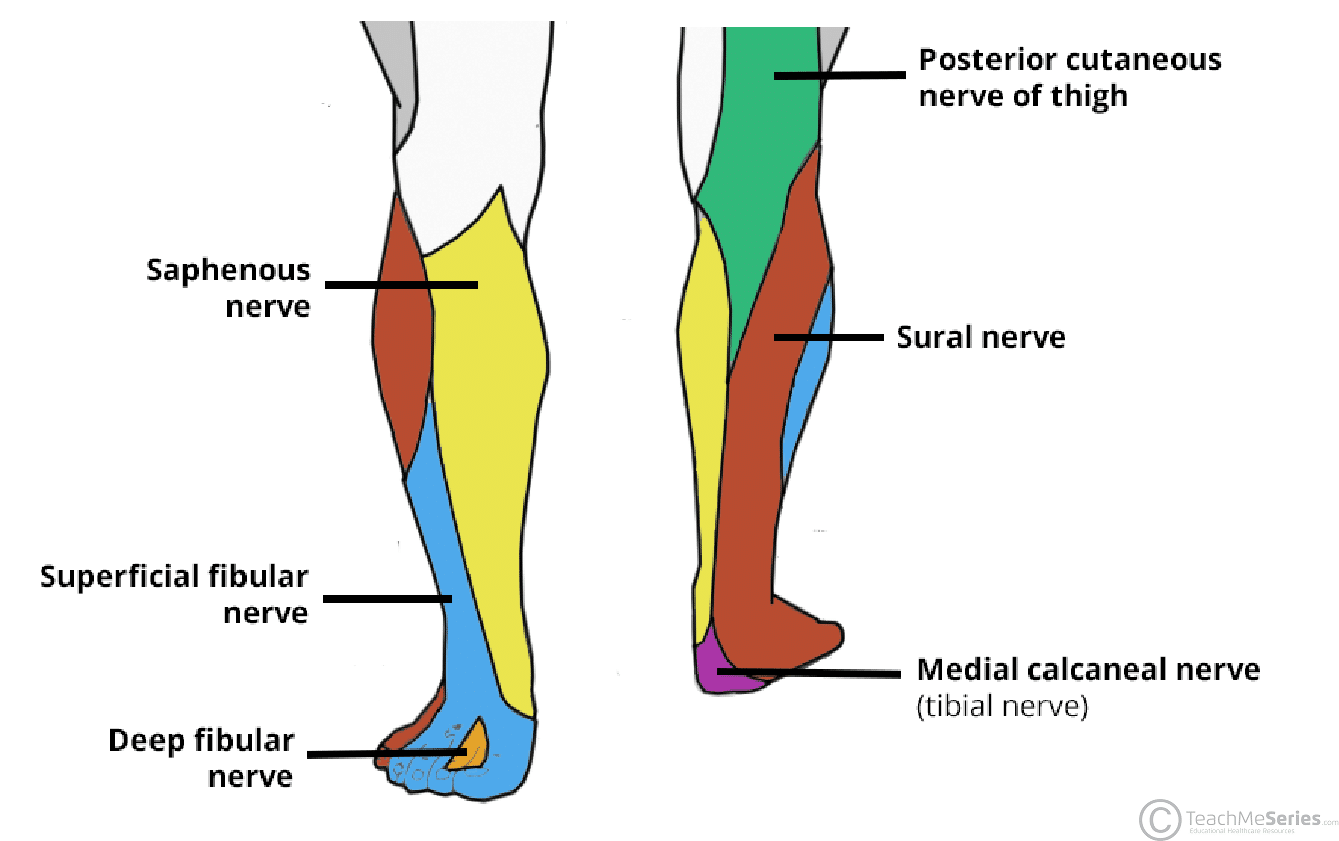
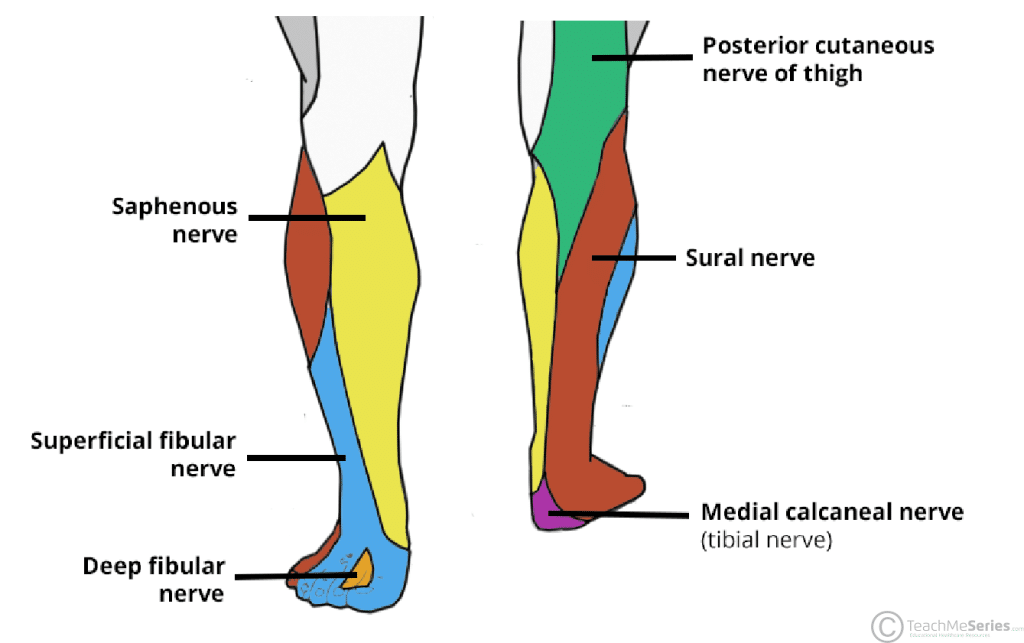
In the popliteal fossa, the tibial nerve gives off cutaneous branches. These combine with branches from the common fibular nerve to form the sural nerve. This sensory nerve innervates the skin of the posterolateral side of the leg and the lateral side of the foot.
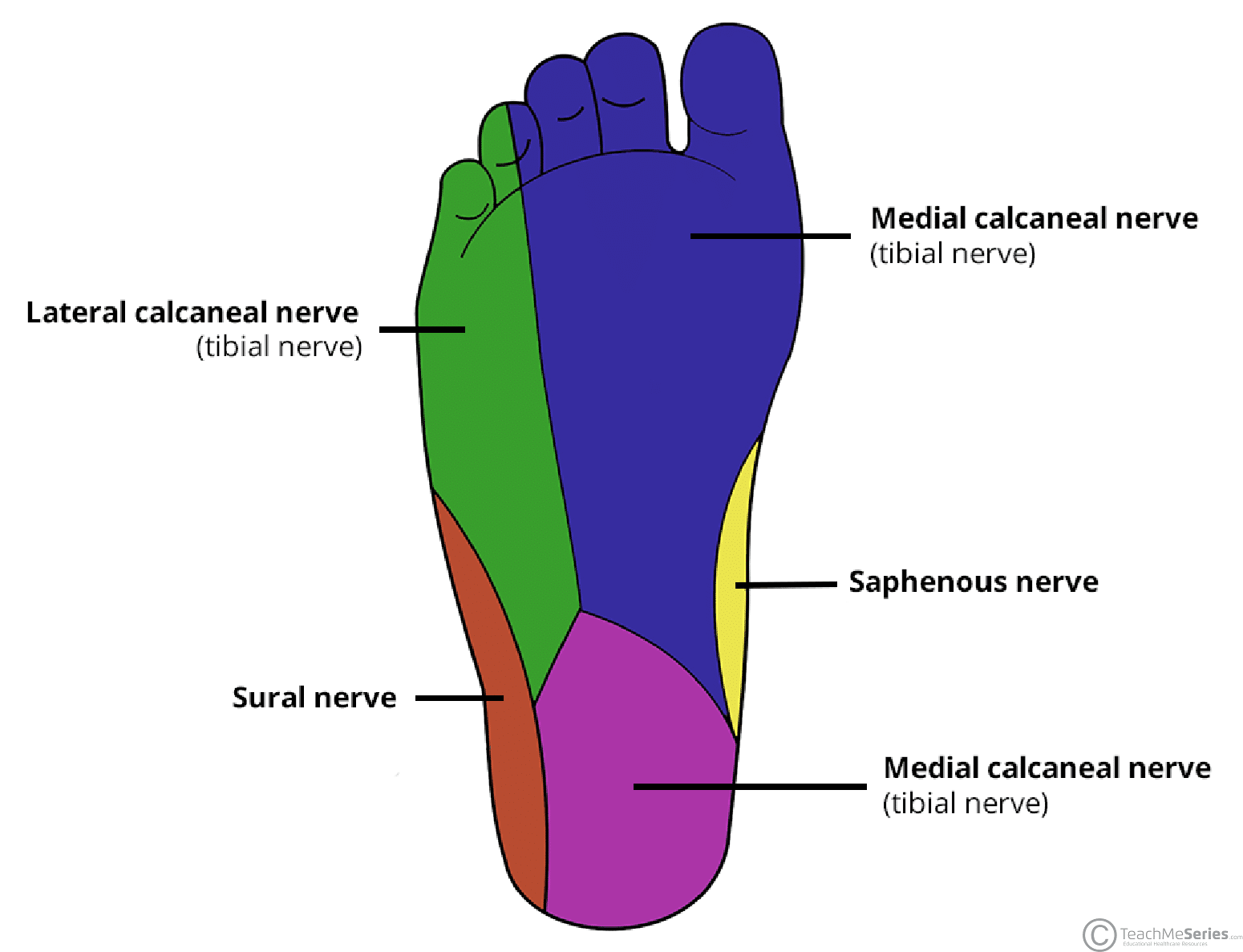
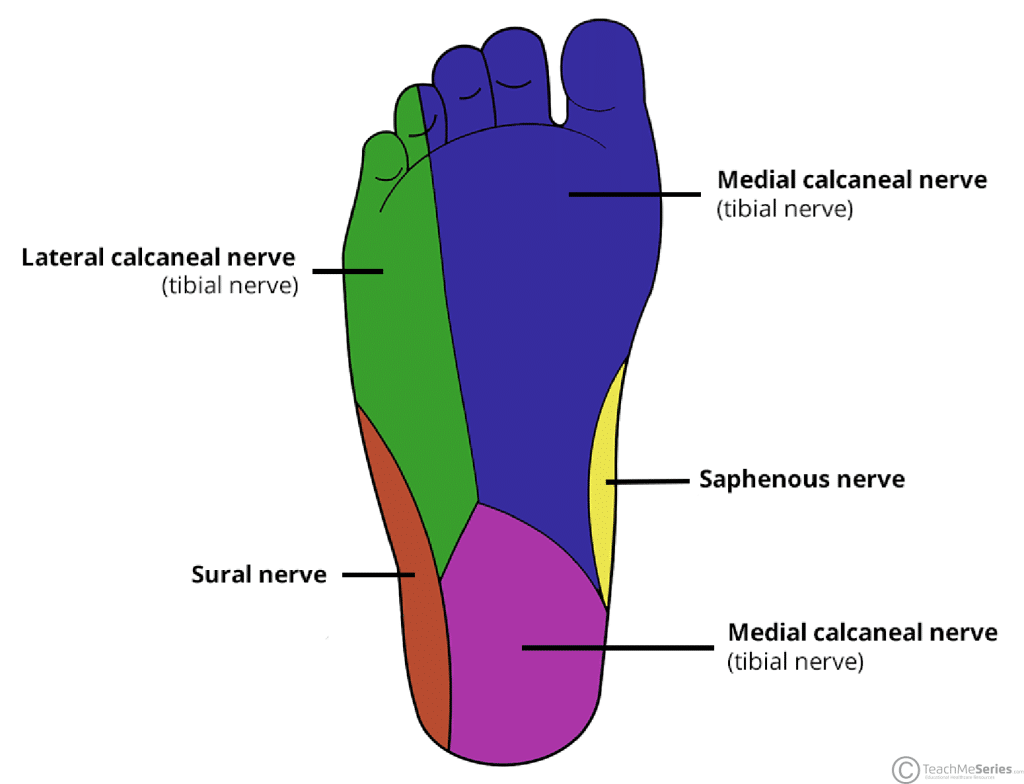
The tibial nerve also supplies all the sole of the foot via three branches:
- Medial calcaneal branches: These arise within the tarsal tunnel, and innervate the skin over the heel.
- Medial plantar nerve: Innervates the plantar surface of the medial three and a half digits, and the associated sole area.
- Lateral plantar nerve: Innervates the plantar surface of the lateral one and a half digits, and the associated sole area.
Clinical Relevance: Damage to the Tibial Nerve
Damage to the tibial nerve is rare, and is often a result of direct trauma, entrapment through narrow space or compression for long period of time. Damage results in loss of plantar flexion, loss of flexion of toes and weakened inversion (The tibialis anterior can still invert the foot).