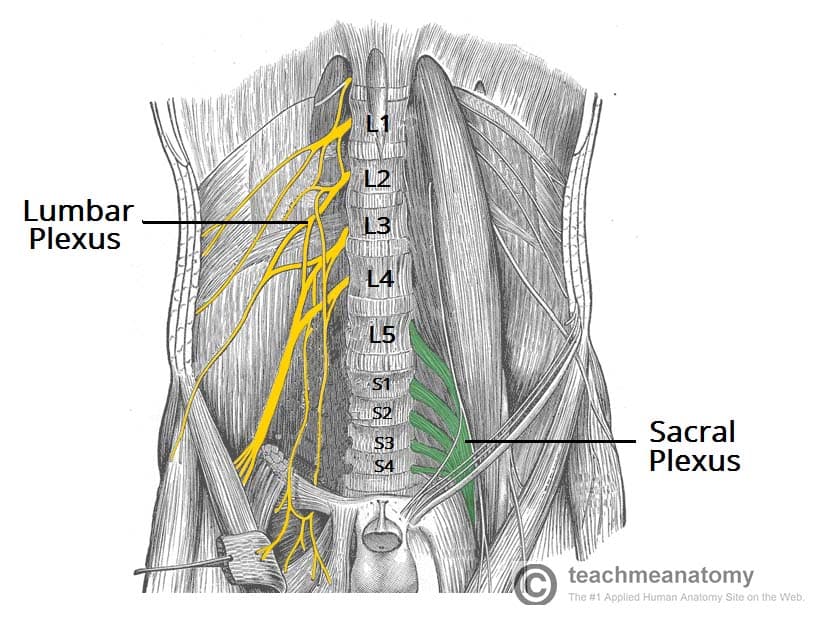
The sacral plexus is a network of nerve fibres that supplies the skin and muscles of the pelvis and lower limb. It is located on the surface of the posterior pelvic wall, anterior to the piriformis muscle.
The plexus is formed by the anterior rami (divisions) of the sacral spinal nerves S1, S2, S3 and S4. It also receives contributions from the lumbar spinal nerves L4 and L5.
In this article, we shall look at the anatomy of the sacral plexus – its formation and major branches.
Spinal Nerves
The spinal nerves S1 – S4 form the basis of the sacral plexus.
At each vertebral level, paired spinal nerves leave the spinal cord via the intervertebral foramina of the vertebral column.
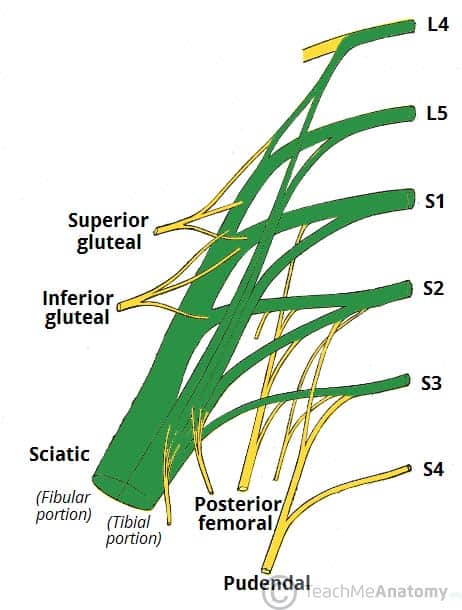
Each nerve then divides into anterior and posterior nerve fibres. The sacral plexus begins as the anterior fibres of the spinal nerves S1, S2, S3, and S4. They are joined by the 4th and 5th lumbar roots, which combine to form the lumbosacral trunk. This descends into the pelvis to meet the sacral roots as they emerge from the spinal cord.
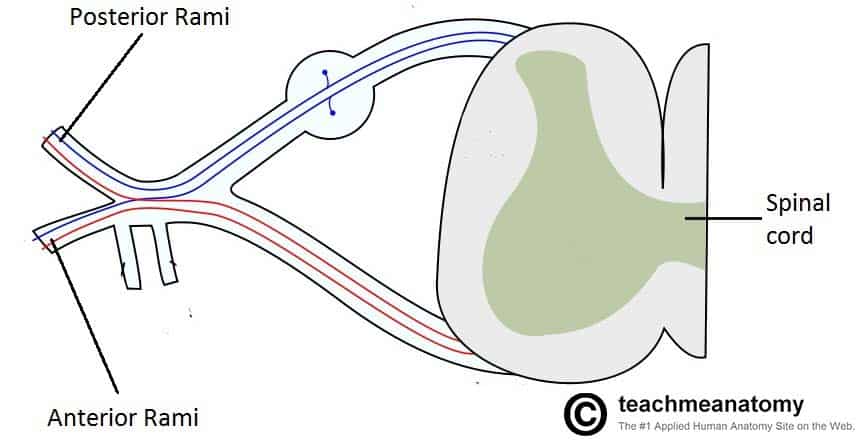
Fig 1 – The spinal cord outflow at each vertebral level. The anterior rami of vertebral levels S1-S4 make up the roots of the sacral plexus.
The Branches
The anterior rami of the S1-S4 spinal roots (and the lumbosacral trunk) divide into several cords. These cords then combine together to form the five major peripheral nerves of the sacral plexus.
These nerves then descend down the posterior pelvic wall. They have two main destinations:
- Leave the pelvis via the greater sciatic foramen – these nerves enter the gluteal region of the lower limb, innervating the structures there.
- Remain in the pelvis – these nerves innervate the pelvic muscles, organs and perineum.
We shall now consider the branches of the sacral plexus.
(Note: In this article we shall include only brief notes on the function of these nerves – for more detailed information click on the title to visit their respective pages)
Superior Gluteal Nerve
The superior gluteal nerve leaves the pelvis via the greater sciatic foramen, entering the gluteal region superiorly to the piriformis muscle. It is accompanied by the superior gluteal artery and vein for much of its course.
Roots: L4, L5, S1.
Motor Functions: Innervates the gluteus minimus, gluteus medius and tensor fascia lata.
Sensory Functions: None.
A useful memory aid for the major branches of the sacral plexus is ‘Some Irish Sailor Pesters Polly’. This stands for Superior Gluteal, Inferior Gluteal, Sciatic, Posterior cutaneous nerve of thigh, Pudendal.
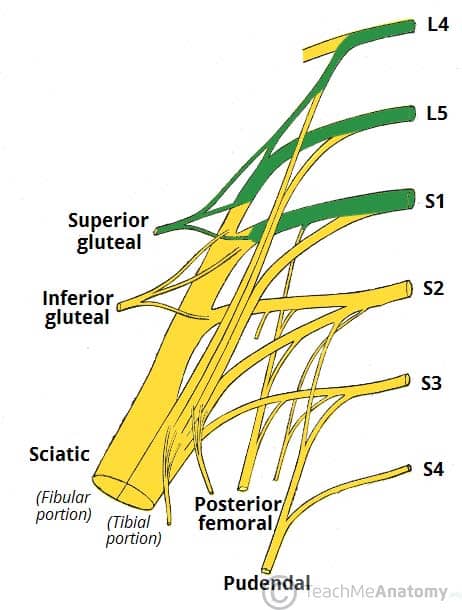
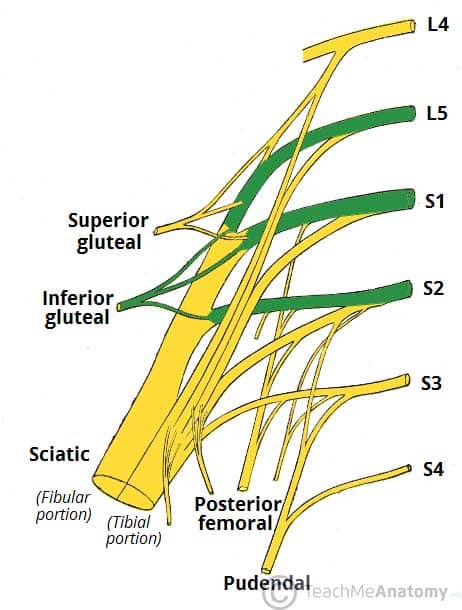
Inferior Gluteal Nerve
The inferior gluteal nerve leaves the pelvis via the greater sciatic foramen, entering the gluteal region inferiorly to the piriformis muscle.
It is accompanied by the inferior gluteal artery and vein for much of its course.
Roots: L5, S1, S2.
Motor Functions: Innervates gluteus maximus.
Sensory Functions: None.
Sciatic Nerve
See more detailed information here
- Roots: L4, L5, S1, S2, S3
- Motor Functions:
- Tibial portion – Innervates the muscles in the posterior compartment of the thigh (apart from the short head of the biceps femoris), and the hamstring component of adductor magnus. Innervates all the muscles in the posterior compartment of the leg and sole of the foot.
- Common fibular portion – Short head of biceps femoris, all muscles in the anterior and lateral compartments of the leg and extensor digitorum brevis.
- Sensory Functions:
- Tibial portion: supplies the skin of the posterolateral leg, lateral foot and the sole of the foot.
- Common fibular portion: supplies the skin of the lateral leg and the dorsum of the foot.
For more details about the Tibial nerve, click here.
For more details about the Common Fibular nerve, click here.
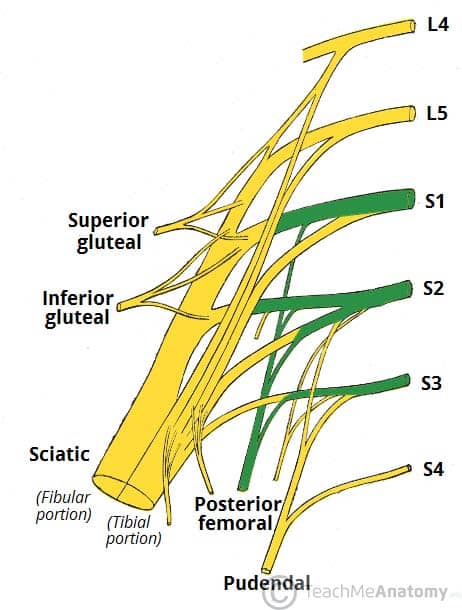
Posterior Femoral Cutaneous
The posterior cutaneous nerve of thigh leaves the pelvis via the greater sciatic foramen, entering the gluteal region inferiorly to the piriformis muscle. It descends deep to the gluteus maximus and runs down the back of the thigh to the knee.
Roots: S1, S2, S3
Motor Functions: None
Sensory Functions: Innervates the skin on the posterior surface of the thigh and leg. Also innervates the skin of the perineum.
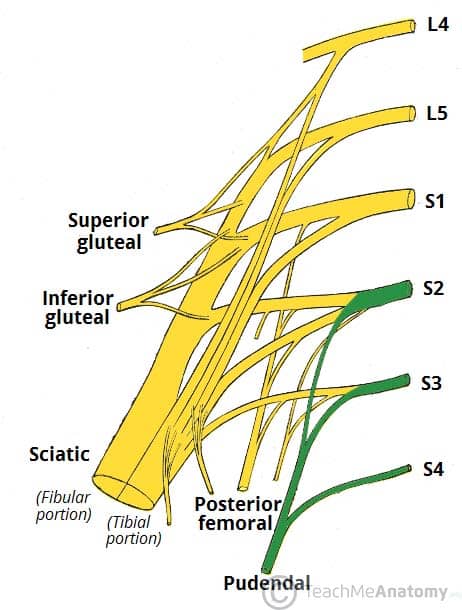
Pudendal Nerve
This nerve leaves the pelvis via the greater sciatic foramen, then re-enters via the lesser sciatic foramen. It moves anterosuperiorly along the lateral wall of the ischiorectal fossa, and terminates by dividing into several branches.
Roots: S2, S3, S4
Motor Functions: Innervates the skeletal muscles in the perineum, the external urethral sphincter, the external anal sphincter, levator ani.
Sensory Functions: Innervates the penis and the clitoris and most of the skin of the perineum.
(Tip – an easy way to remember the functions of the pudendal nerve is S2, S3, S4 keeps poo off the floor!)
Other Branches
In addition to the five major nerves of the sacral plexus, there are a number of smaller branches. These tend to be nerves that directly supplying muscles (with the exception of the perforating cutaneous nerve, which supplies the skin over the inferior gluteal region and the pelvic splanchnic nerves, which innervate the abdominal viscera):
- Nerve to piriformis
- Nerve to obturator internus
- Nerve to quadratus femoris
Clinical Relevance – Lumbosacral Plexopathy
A lumbosacral plexopathy is a disorder affecting either the lumbar or sacral plexus of nerves. They are rare syndromes, caused by damage to the nerve bundles.
A plexopathy is suspected if the symptoms cannot be localised to a single nerve. Patients may complain of neuropathic pains, numbness or weakness and wasting of muscles.
One of the main causes of lumbosacral plexopathy is diabetic amyotrophy, also known as lumbosacral radioplexus neurophagy. In this condition, the high blood sugar levels damage the nerves. Idiopathic plexopathy is another cause, being the lumbosacral equivalent of Parsonage-Turner syndrome (which affects the brachial plexus). Tumours and other local invasions can cause the plexopathy due to the compression of the plexus.
Treatment depends on what is causing the symptoms. For tumours and space-occupying lesions, they should be removed if possible. For diabetic and idiopathic causes, treatment with high-dose corticosteroids can be useful.