The gluteal region is an anatomical area located posteriorly to the pelvic girdle, at the proximal end of the femur. The muscles in this region move the lower limb at the hip joint.
The muscles of the gluteal region can be broadly divided into two groups:
- Superficial abductors and extenders – group of large muscles that abduct and extend the femur. Includes the gluteus maximus, gluteus medius, gluteus minimus and tensor fascia lata.
- Deep lateral rotators – group of smaller muscles that mainly act to laterally rotate the femur. Includes the quadratus femoris, piriformis, gemellus superior, gemellus inferior and obturator internus.
The arterial supply to these muscles is mostly via the superior and inferior gluteal arteries – branches of the internal iliac artery. Venous drainage follows the arterial supply.
In this article, we shall examine the two groups of gluteal muscles – their attachments, innervations and actions. We shall also look at the clinical consequence of gluteal muscle disorders.
The Superficial Muscles
The superficial muscles in the gluteal region consist of the three glutei and the tensor fascia lata. They mainly act to abduct and extend the lower limb at the hip joint.
Gluteus Maximus
The gluteus maximus is the largest of the gluteal muscles. It is also the most superficial, producing the shape of the buttocks.
- Attachments: Originates from the gluteal (posterior) surface of the ilium, sacrum and coccyx. The fibres slope across the buttock at a 45 degree angle and insert onto the iliotibial tract and gluteal tuberosity of the femur.
- Actions: It is the main extensor of the thigh, and assists with lateral rotation. However, it is only used when force is required, such as running or climbing.
- Innervation: Inferior gluteal nerve.
By TeachMeSeries Ltd (2024)
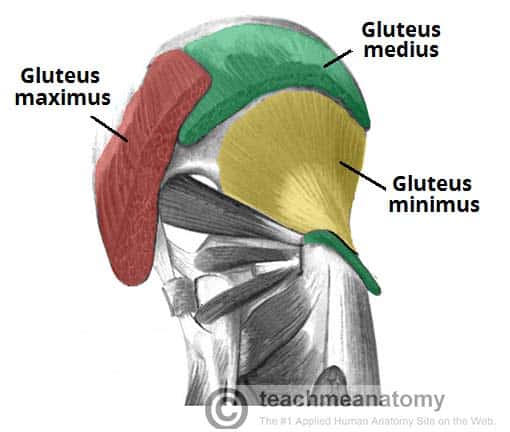
Fig 1 – The superficial muscles of the gluteal region. The gluteus maximus and medius have been partly removed.
Gluteus Medius
The gluteus medius muscle is fan-shaped and lies between to the gluteus maximus and the minimus. It is similar in shape and function to the gluteus minimus.
- Attachments: Originates from the gluteal surface of the ilium and inserts into the lateral surface of the greater trochanter.
- Actions: Abduction and medial rotation of the lower limb. It stabilises the pelvis during locomotion, preventing ‘dropping’ of the pelvis on the contralateral side.
- Innervation: Superior gluteal nerve.
Gluteus Minimus
The gluteus minimus is the deepest and smallest of the superficial gluteal muscles. It is similar in shape and function to the gluteus medius.
- Attachments: Originates from the ilium and converges to form a tendon, inserting to the anterior side of the greater trochanter.
- Actions: Abduction and medial rotation of the lower limb. It stabilises the pelvis during locomotion, preventing ‘dropping’ of the pelvis on the contralateral side.
- Innervation: Superior gluteal nerve.
Tensor Fascia Lata
Tensor fasciae lata is a small superficial muscle which lies towards the anterior edge of the iliac crest. It functions to tighten the fascia lata, and so abducts and medially rotates the lower limb.
- Attachments: Originates from the anterior iliac crest, attaching to the anterior superior iliac spine (ASIS). It inserts into the iliotibial tract, which itself attaches to the lateral condyle of the tibia.
- Actions: Assists the gluteus medius and minimus in abduction and medial rotation of the lower limb. It also plays a supportive role in the gait cycle.
- Innervation: Superior gluteal nerve.
Clinical Relevance: Damage to the Superior Gluteal Nerve
The superior gluteal nerve innervates the gluteus medius and the gluteus minimus. These muscles have an important role in stabilising the pelvis during locomotion. In the standing position, the gluteus minimus and medius contract when the contralateral leg is raised, preventing the pelvis from dropping on that side.
If the superior gluteal nerve is damaged, the previously described muscles are paralysed – and the pelvis becomes unsteady. A characteristic finding of gluteal muscle weakness is the Trendelenburg sign.
Trendelenburg Sign
The Trendelenburg sign is produced when the patient is asked to stand unassisted on each leg in turn. In a positive sign, pelvic drop will occur on the unsupported leg. Pelvic drop can be recognised by observing the level of the iliac crests on both sides.
For example, if the left gluteal muscles are weak, the right side of the pelvis will drop when the patient stands on their left leg (and the right leg is unsupported).
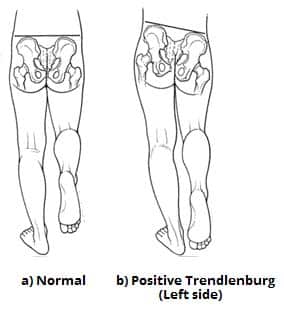
Fig 2 – Positive Trendelenburg sign, characteristic of left superior gluteal nerve palsy.
The Deep Muscles
The deep gluteal muscles are a set of smaller muscles, located underneath the gluteus minimus. The general action of these muscles is to laterally rotate the lower limb. They also stabilise the hip joint by ‘pulling’ the femoral head into the acetabulum of the pelvis.
Piriformis
The piriformis muscle is a key landmark in the gluteal region. It is the most superior of the deep muscles.
- Attachments: Originates from the anterior surface of the sacrum. The fibres travel inferiorly and laterally through the greater sciatic foramen to insert onto the greater trochanter of the femur.
- Actions: Lateral rotation and abduction.
- Innervation: Nerve to piriformis.
Obturator Internus
The obturator internus forms the lateral walls of the pelvic cavity. In some texts, the obturator internus and the gemelli muscles are considered as one muscle – the triceps coxae.
- Attachments: Originates from the pubis and ischium at the obturator foramen. It travels through the lesser sciatic foramen, and attaches to the greater trochanter of the femur.
- Actions: Lateral rotation and abduction.
- Innervation: Nerve to obturator internus.
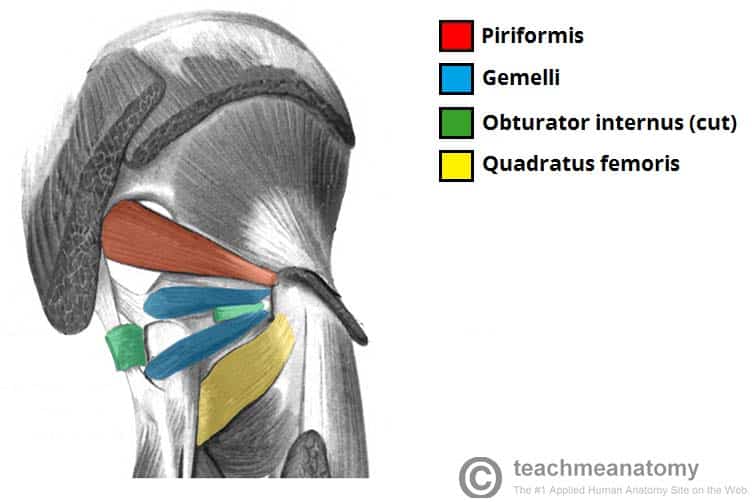
The Gemelli – Superior and Inferior
The gemelli are two narrow and triangular muscles. They are separated by the obturator internus tendon.
- Attachments: The superior gemellus muscle originates from the ischial spine, the inferior from the ischial tuberosity. They both attach to the greater trochanter of the femur.
- Actions: Lateral rotation and abduction.
- Innervation: The superior gemellus muscle is innervated by the nerve to obturator internus, the inferior gemellus is innervated by the nerve to quadratus femoris.
Quadratus Femoris
The quadratus femoris is a flat, square-shaped muscle. It is the most inferior of the deep gluteal muscles, located below the gemelli and obturator internus.
- Attachments: Originates from the lateral aspect of the ischial tuberosity and attaches to the quadrate tuberosity on the intertrochanteric crest.
- Actions: Lateral rotation.
- Innervation: Nerve to quadratus femoris.
Clinical Relevance: Landmark of the Gluteal Region
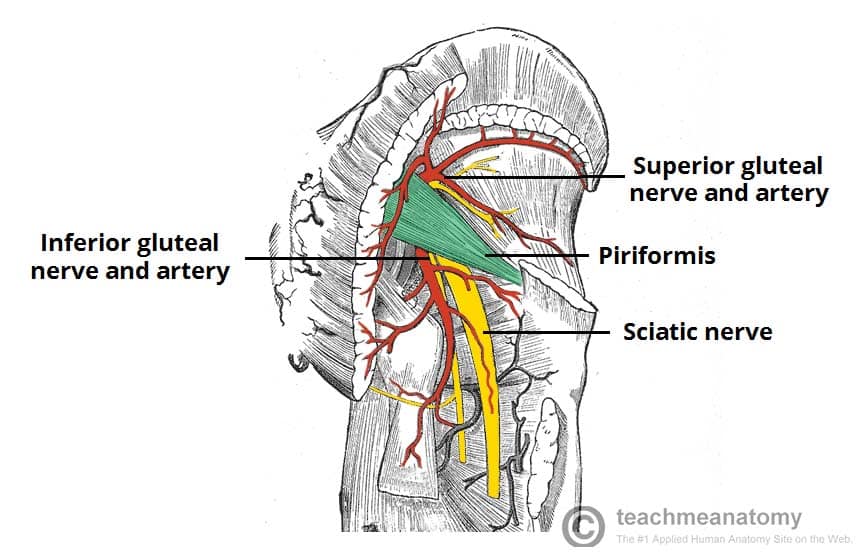
The piriformis is an important anatomical landmark in the gluteal region.
As the muscle travels through the greater sciatic foramen, it effectively divides the gluteal region into an inferior and superior part. This division determines the name of the vessels and nerves that supply the area. The superior gluteal nerve and vessels emerge into the gluteal region superiorly to the piriformis (and vice versa for the inferior gluteal nerve).
In addition, the piriformis can be used to locate the sciatic nerve (a major peripheral nerve of the lower limb). The sciatic nerve enters the gluteal region directly inferior to the piriformis, and is visible as a flat band, approximately 2cm wide.