The hypoglossal nerve is the twelfth paired cranial nerve.
Its name is derived from ancient Greek, ‘hypo‘ meaning under, and ‘glossal‘ meaning tongue. The nerve has a purely somatic motor function, innervating all the extrinsic and intrinsic muscles of the tongue (except the palatoglossus, innervated by vagus nerve).
In this article, we shall look at the anatomy of the hypoglossal nerve – its anatomical course, motor functions and clinical correlations.
Anatomical Course
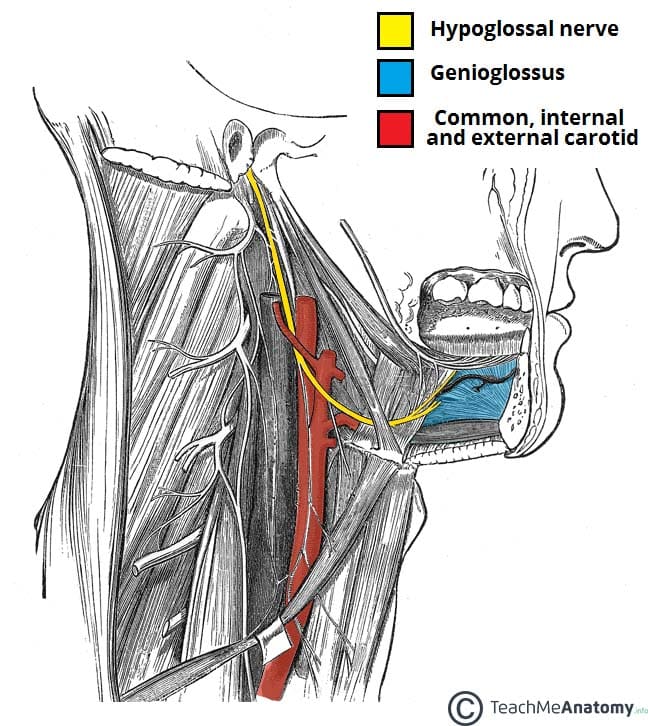
The hypoglossal nerve arises from the hypoglossal nucleus in the medulla oblongata of the brainstem. It then passes laterally across the posterior cranial fossa, within the subarachnoid space. The nerve exits the cranium via the hypoglossal canal of the occipital bone.
Now extracranial, the nerve receives a branch of the cervical plexus that conducts fibres from C1/C2 spinal nerve roots. These fibres do not combine with the hypoglossal nerve – they merely travel within its sheath.
It then passes inferiorly to the angle of the mandible, crossing the internal and external carotid arteries, and moving in an anterior direction to enter the tongue.
Motor Function
The hypoglossal nerve is responsible for motor innervation of the vast majority of the muscles of the tongue (except for palatoglossus). These muscles can be subdivided into two groups:
i) Extrinsic muscles
- Genioglossus (makes up the bulk of the tongue)
- Hyoglossus
- Styloglossus
- Palatoglossus (innervated by vagus nerve)
ii) Intrinsic muscles
- Superior longitudinal
- Inferior longitudinal
- Transverse
- Vertical
Together, these muscles are responsible for all movements of the tongue.
Role of the C1/C2 Roots
The C1/C2 roots that travel with the hypoglossal nerve also have a motor function. They branch off to innervate the geniohyoid (elevates the hyoid bone) and thyrohyoid (depresses the hyoid bone) muscles.
Another branch containing C1/C2 fibres descends to supply the ansa cervicalis – a loop of nerves that is part of the cervical plexus. From the ansa cervicalis, nerves arise to innervate the omohyoid, sternohyoid and sternothyroid muscles. These muscles all act to depress the hyoid bone.

Clinical Relevance
Cranial Nerve Examination
The hypoglossal nerve is examined by asking the patient to protrude their tongue.
Other movements such as asking the patient to push their tongue against their cheek and feeling for the pressure on the opposite side of the cheek may also be used if damage is suspected.
Hypoglossal Nerve Palsy
Damage to the hypoglossal nerve is a relatively uncommon cranial nerve palsy. Possible causes include head & neck malignancy and penetrating traumatic injuries. If the symptoms are accompanied by acute pain, a possible cause may be dissection of the internal carotid artery.
Patients will present with deviation of the tongue towards the damaged side on protrusion, as well as possible muscle wasting and fasciculations (twitching of isolated groups of muscle fibres) on the affected side.
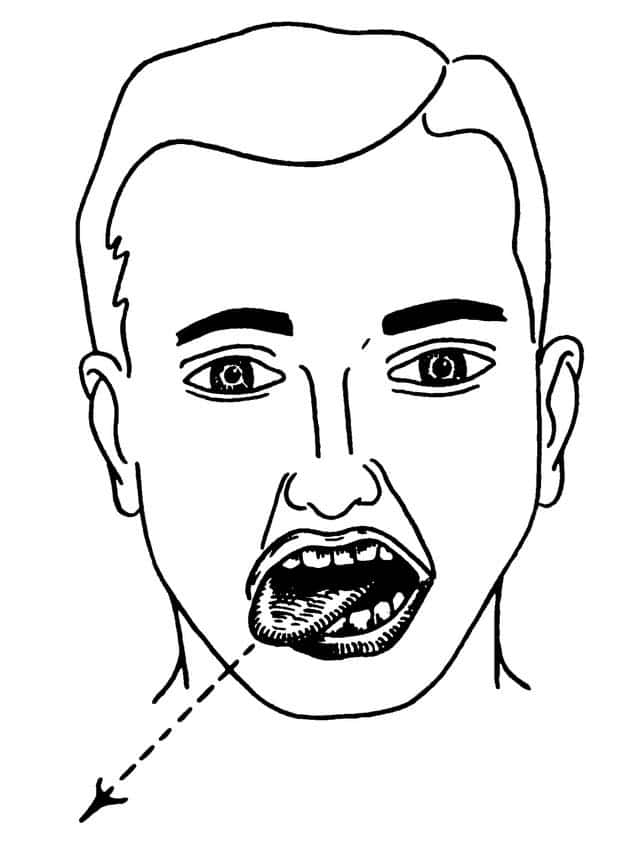
Fig 3 – Right hypoglossal nerve palsy, characterised by deviation of the tongue to the right.