The coeliac trunk is a major artery of the abdomen. It arises from the abdominal aorta, and supplies many of the gastrointestinal viscera.
In this article, we shall look at the anatomy of the coeliac trunk – its anatomical position, branches, anastomoses, and clinical relevance.
Anatomical Position
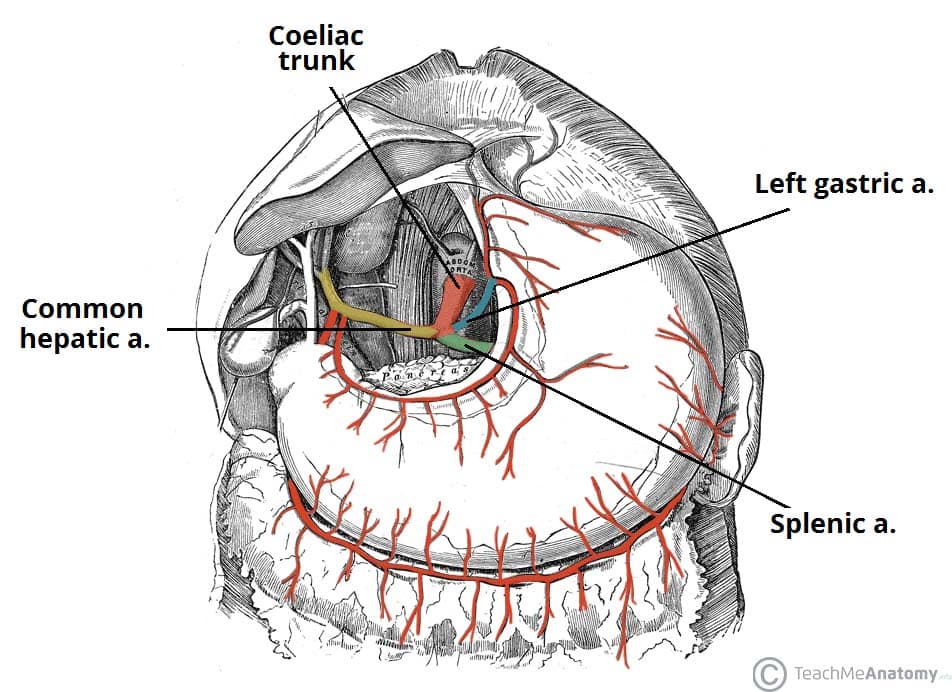
The coeliac trunk is the second branch of the abdominal aorta (the first branches are the paired inferior phrenic arteries). It arises from the anterior aspect of the aorta, at the aortic hiatus of the diaphragm (T12 level).
Major Branches
After emerging from the aorta, the coeliac trunk extends approximately 1cm before dividing into three major branches – left gastric, splenic and common hepatic arteries.
Of these branches, two go left and one goes to the right-hand side. Collectively, they are the major arterial supply to the stomach, spleen, liver, gall bladder, abdominal oesophagus, pancreas and duodenum.
Left Gastric Artery
The left gastric artery is the smallest of the three branches. It ascends across the diaphragm, giving rise to oesophageal branches, before continuing anteriorly along the lesser curvature of the stomach. Here, it anastomoses with the right gastric artery.
Splenic Artery
The splenic artery arises from the coeliac trunk just inferior to the left gastric artery. It then travels left towards the spleen, running posterior to the stomach and along the superior margin of the pancreas. During its course, it is contained within the splenorenal ligament. It terminates into five branches which supply the segments of the spleen.
In addition to supplying the spleen, the splenic artery also gives rise to several important vessels:
- Left gastroepiploic: supplies the greater curvature of the stomach. Anastomoses with the right gastroepiploic artery.
- Short gastrics: 5-7 small branches supplying the fundus of the stomach.
- Pancreatic branches: supply the body and tail of the pancreas.
The splenic artery has a tortuous appearance (similar to the facial branch of the external carotid artery) and thus is easily identifiable from other nearby vessels.
Common Hepatic Artery
The common hepatic artery is the sole arterial supply to the liver and the only branch of the coeliac artery to pass to the right.
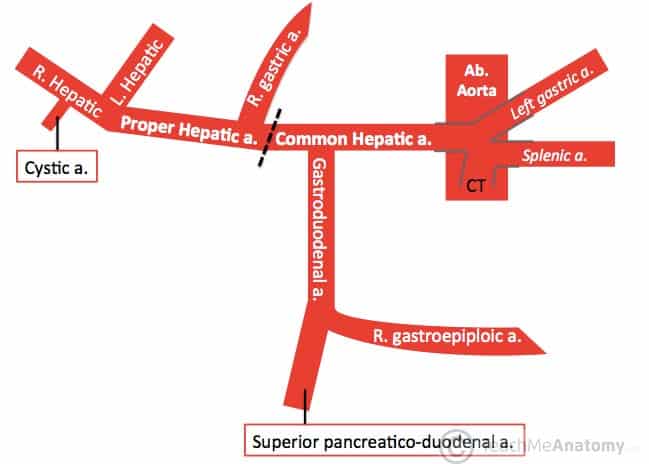
As it travels past the superior aspect of the duodenum, it divides into its two terminal branches – the proper hepatic and gastroduodenal arteries. Each of these arteries has multiple branches and variation in the arrangement of these branches is common.
Proper Hepatic
The proper hepatic artery ascends through the lesser omentum towards the liver. It gives rise to:
- Right gastric: supplies the pylorus and lesser curvature of the stomach.
- Right and left hepatic: divide inferior to the porta hepatis and supply their respective lobes of the liver.
- Cystic: branch of the right hepatic artery – supplies the gall bladder.
Gastroduodenal
The gastroduodenal artery descends posterior to the superior portion of the duodenum. Its branches are:
- Right gastroepiploic: supplies the greater curvature of the stomach. Found between the layers of the greater omentum, which it also supplies.
- Superior pancreaticoduodenal: divides into an anterior and posterior branch, which supplies the head of the pancreas.
Anastomoses
Stomach
The stomach is the only organ to receive arterial supply from the three branches of the coeliac trunk (left gastric, splenic and common hepatic arteries).
This is achieved through a system of anastomoses along the greater (gastroepiploic arteries) and lesser (gastric arteries) curvatures of the stomach.
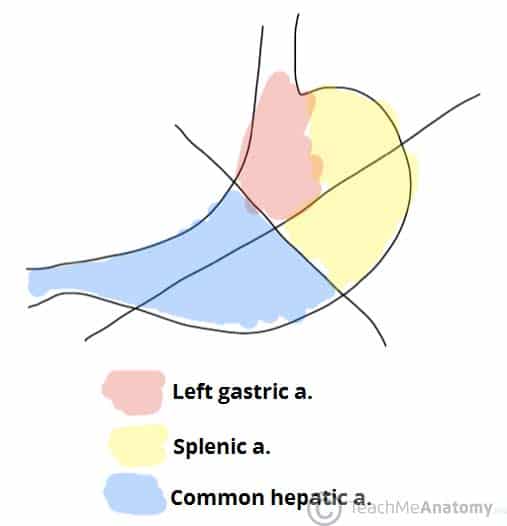
Fig 3 – Schematic demonstrating the relative contributions of each branch of the coeliac trunk to the blood supply of the stomach
Pancreas
The pancreaticoduodenal arcade is a network of arteries that surround and supply the head of the pancreas.
There are two main arteries – each has an anterior and posterior branch, that anastomose (e.g. anterior to anterior) forming a ring structure:
- Superior pancreaticoduodenal– a branch of the gastroduodenal artery.
- Inferior pancreaticoduodenal – branch of superior mesenteric artery (SMA).
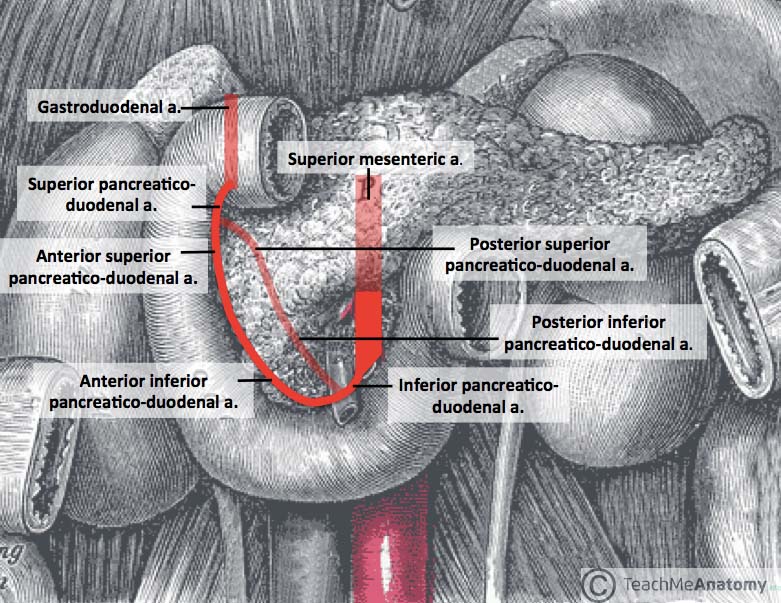
Fig 4 – The pancreaticoduodenal arcade. Note: transparent arteries are posterior to the pictured structures
Clinical Relevance – Disorders of the Coeliac Trunk
Peptic Ulcers
Peptic ulcers in the stomach and duodenum have potential to cause significant gastrointestinal bleeding if they erode into neighbouring arteries (usually the gastroduodenal artery).
Coeliac Trunk Compression Syndrome
The median arcuate ligament (the fibrous anchor of the diaphragm that forms the aortic hiatus) occasionally lies anterior to the coeliac trunk, rather than its usual superior position.
This can cause compression of the coeliac trunk that may present pathologically as pain. The pain is thought to be caused by the resulting ischemia of the abdominal organs -though it also may be associated with compression of the coeliac ganglia.
The treatment of coeliac trunk compression syndrome is the surgical division of the median arcuate ligament.

Fig 5 – Coeliac trunk compression syndrome.
Splenic Artery Aneurysm
Splenic artery aneurysms are the most common type of visceral aneurysm, comprising around 60% of the total.
The main risk factors for their development are female sex, multiple pregnancies, portal hypertension, and pancreatitis or pancreatic pseudocyst formation.
Those that are symptomatic will present with a vague epigastric or LUQ pain. Those that rupture will present with severe abdominal pain and haemodynamic compromise.
First line management option is endovascular repair; this is best done with embolisation or stent grafts, once the patient is haemodynamically stable (an open repair may be advised in the unstable patient).
Variations
The arrangement of the branches and the order from which they arise from the coeliac trunk can vary from person to person. This is important to remember when orientating yourself with a specimen. Here are some examples of common variations:
- The left gastric artery often arises proximal to the bifurcation of the splenic and common hepatic arteries. This is called a false tripod.
- The right gastric artery is occasionally seen as a branch of the common hepatic instead of the proper hepatic artery.
- The right gastric and right hepatic arteries may arise from the SMA.
- The left hepatic artery is sometimes seen as a branch of the left gastric artery.
- The inferior phrenic arteries may arise from the coeliac trunk instead of the abdominal aorta